Reading Navigation
Psilocybin for Mental Health


From microdosing to spiritual ceremonies to psychedelic-assisted therapy, you’ve probably heard someone in your circle talking about the healing potential of psilocybin. A naturally occurring compound found in more than 200 species of “magic mushrooms,” psilocybin has been used for centuries in traditional healing contexts and is now the subject of a wave of ongoing clinical research.
This guide takes a deep dive into what we currently know: its history and traditional uses, how it works in the brain, how it is being used in contemporary psychedelic-assisted therapy, potential risks and contraindications, and first-hand accounts from people who have experienced it.

What is Psilocybin?
Even though psilocybin has been used for millennia by Indigenous cultures, with deep roots in ritual and ceremony, Western medicine is only starting to catch up, with a growing body of studies and clinical trials investigating its therapeutic potential.
A naturally occurring tryptamine compound found in more than 200 species of fungi, psilocybin is found most commonly in the Psilocybe genus, which grows across nearly every continent. The potency of psilocybin mushrooms can vary widely depending on the species, even in individual mushrooms, with Psilocybe cubensis being the most well-known. In addition to its natural form, psilocybin can also be synthesized in a laboratory to produce an isolated, precisely dosed compound. This synthetic version is used in clinical settings, allowing for the kind of standardized, controlled dosing that scientific trials require. These days, the term psilocybin is often used loosely to refer to both the mushroom and its pure, synthetic form.
In recent years, headlines like “The Psychedelic Revolution Is Coming. Psychiatry Might Never Be The Same” have heralded the paradigm-shifting possibilities of psychedelic-assisted therapy. Psilocybin-assisted therapy, similar to other psychedelic-assisted therapy protocols, is typically broken down into three phases: preparation, the dosing session, and integration. More than merely ingesting a substance, it involves intensive work with a therapist before and after the dosing session, which usually consists of one or two high doses of psilocybin.
Although psilocybin is what you ingest, once inside the body it is rapidly converted by the liver into psilocin1, which crosses the blood-brain barrier and binds to serotonin receptors to produce the characteristic perceptual, emotional, and visionary effects of the psychedelic experience.
Beyond clinical trials and formal therapy frameworks, psilocybin mushrooms are used in a wide variety of contexts, from legal and underground retreats to festivals, spiritual ceremonies to solo trips. Set and setting matter enormously, with intention, preparation, and support all significantly shaping the experience.
A Brief History of Psilocybin Mushrooms
Although there are over 200 varieties of psilocybin mushrooms that grow around the world, they first entered mainstream Western awareness when former banker and amateur mycologist Gordon Wasson published “Seeking the Magic Mushroom” in Life Magazine in 1957, after sitting in ceremony with Mazatec curandera María Sabina two years earlier.
Wasson was among the first Westerners to document an Indigenous Mazatec ceremony. As the story goes, María Sabina was reluctant to share the ceremony with him, but agreed on the condition that any photos would not be shared with outsiders. Wasson later violated this agreement, and the article went viral, fueling the birth of the American psychedelic counterculture and triggering an influx of spiritual tourists to Huautla.
The consequences for the Mazatec community were devastating. The surge of seekers led to the commercialization of a sacred practice that had traditionally been private, and María Sabina paid a heavy personal price. In her own words, “I realized the young people with long hair didn’t need me to eat the little things. Kids ate them anywhere and anytime, and they didn’t respect our customs.”
This history matters as psilocybin moves into mainstream medicine and wellness culture, with pharmaceutical companies seeking to develop patents while the communities who stewarded these traditions rarely see benefit or compensation2.
Wasson’s article prompted people world over to realise that psychedelic fungi were more prevalent than they thought, leading thinkers like Terence McKenna to theorize that humans evolved larger brains through consuming psychoactive mushrooms, though no conclusive evidence exists for this.
In 1958, Swiss chemist Albert Hofmann became the first to isolate psilocybin and psilocin from the mushroom Psilocybe mexicana. Hofmann had previously discovered LSD, another psychedelic being investigated for therapeutic use. With LSD sessions lasting up to 12 hours3, Hofmann’s employer, Sandoz, was keen to find a shorter-acting alternative.
After isolating psilocybin, Hofmann developed a synthetic version branded Indocybin, testing it on himself first. Sandoz then distributed it to physicians and clinicians globally for use in therapy, selling it from 1961 until 1966, when mounting cultural backlash prompted them to discontinue. Psilocybin was later classified as a Schedule I controlled substance under the 1971 United Nations Convention on Psychotropic Substances, defined as having “no currently accepted medical use in treatment.”


In 1960, Harvard psychologist Timothy Leary traveled to Mexico after reading Wasson’s article, seeking a mushroom experience of his own. What followed transformed his life and shattered his worldview. Recounting his journey he shared, “I learned more about psychology in the five hours after taking these mushrooms than I had in the preceding 15 years of studying and researching psychology.”
Back at Harvard, Leary secured psilocybin from Sandoz and co-founded the Harvard Psilocybin Project with Richard Alpert (later Ram Dass), exploring whether psilocybin could reduce reoffending in prison inmates (Concord Prison Experiment) and spark genuine religious experiences in divinity students (Marsh Chapel Good Friday Experiment). Though results were promising, the research was criticized for lacking rigor, and both men were eventually fired after word spread that they were experimenting on themselves and encouraging students to do the same.
Leary went on to become the face of the 1960s psychedelic counterculture, urging millions to “Turn on, tune in, and drop out.” President Nixon famously called him “the most dangerous man in America,” and in 1970 psilocybin was made illegal alongside LSD under the Controlled Substances Act.
More than four decades later, a new wave of clinical research has emerged. In 2018, the FDA granted psilocybin Breakthrough Therapy status for both treatment-resistant depression and major depressive disorder, fast-tracking its development and review as a potential treatment.
How Does Psilocybin Work?
Psilocybin is a classic psychedelic4 that works by binding to serotonin 5-HT2A receptors in the brain. Densely concentrated in the prefrontal cortex, these receptors are associated with mood regulation, sense of self, rumination, and higher-order thinking.
From childhood to adulthood, our brains develop habitual pathways of communication between regions that tend to solidify over time5. Psilocybin is thought to disrupt this, heightening communication between brain regions that don’t typically connect, increasing neuroplasticity, and helping to break rigid patterns of thought.
One of its most significant effects is on the brain’s default mode network (DMN), the system linked to our narrative sense of self, self-reflection, and self-criticism, which tends to be overactive in conditions like depression6, anxiety7, and OCD8. When you ingest psilocybin, DMN activity is significantly reduced9 while connectivity in other regions increases, thought to help abate negative thought patterns, increase psychological flexibility10, and contribute to the well-known experience of ego-dissolution11.
Ego-dissolution, sometimes called ego death, can feel like a genuine experience of dying, involving the temporary erosion of one’s subjective, biographical sense of self. It can be both ecstatic and terrifying, and constitutes a type of mystical or unitive experience in which the boundary between self and world dissolves, giving rise to feelings of deep interconnectedness and a merging with something larger than oneself.
A landmark 2006 study12 from Johns Hopkins showed that psilocybin can reliably produce these kinds of mystical experiences, with more than 70% of participants rating their session as one of the five most meaningful and spiritually significant experiences of their lives. Later research confirmed that the intensity of the mystical experience positively correlated with therapeutic outcomes.
Beyond neuroscience, Indigenous cultures have long understood mushrooms not as mere molecules but as living, sentient intelligences capable of communicating with us. This felt sense of encountering a distinct presence or guiding intelligence is reported by many people across many contexts, and points to something about psilocybin’s healing capacity that remains difficult to capture in clinical contexts alone.

Psilocybin Uses in Therapy
Psilocybin has gained significant clinical attention for its potential to help with depression, existential anxiety in life-threatening illness, substance use disorders, and a variety of other less common conditions such as cluster headaches13, chronic pain14, and post-treatment Lyme disease, to name but a few.
Psilocybin for Depression
The use of psilocybin as a treatment for depression is one of the most common clinical uses of the substance, with the FDA having granted psilocybin Breakthrough Therapy status for both treatment-resistant depression and major depressive disorder.
A Johns Hopkins study found that just two doses of psilocybin combined with psychotherapy produced rapid reductions in depressive symptoms, with 54% of participants in remission after four weeks. A 2022 follow-up15 found most participants still maintained those gains a full year later.
Another study16 by researchers at Imperial College London compared two doses of psilocybin against six weeks of daily escitalopram, one of the most widely prescribed antidepressants, in patients with moderate to severe depression, finding remission rates were twice as high in the psilocybin group (57% versus 28%). A six-month follow-up17 found that psilocybin and escitalopram performed similarly over time, however, those who had received psilocybin improved in other ways not specifically measured by symptom remission, including enhanced functioning, connectedness, and greater meaning in life.
In 2022, a large international phase 2 trial18 involving 233 patients with treatment-resistant depression across multiple sites found that a single 25mg dose of psilocybin produced significant reductions in depression scores compared to a control dose, sustained for at least six weeks. The following year, a multisite randomized controlled trial19 involving 104 adults with major depressive disorder found that a single 25mg dose of psilocybin alongside psychological support produced rapid antidepressant effects, sustained reductions in depressive symptoms, and improvements in psychosocial functioning compared to placebo.


Psilocybin for End-of-Life Distress
For individuals facing life-threatening or terminal illness such as cancer, the psychological weight can be equally as devastating as the physical one, leading to anxiety, depression, demoralization, and a collapse of meaning. Researchers at Johns Hopkins published a 2016 landmark study20, administering a single high dose (22 or 30 mg, adjusted for body weight) to cancer patients found that six months after around 80% showed clinically significant reductions in depression and anxiety, reporting a greater ability to cope with their fear of death and a renewed sense of meaning. Seventy percent of participants rated their experience to be among the top five most personally meaningful experiences of their lives, with the degree to which a person had a mystical experience correlating with measured therapeutic benefit.
Separately, NYU researchers21 found that psilocybin-assisted therapy significantly reduced suicidal ideation in cancer patients, with effects appearing as early as eight hours after dosing and lasting up to 4.5 years in follow-up, a finding with profound implications given how limited existing options are for suicidality in this population.
In reflecting on how psilocybin helped alleviate anxiety in patients, the late Johns Hopkins psychiatrist and psilocybin pioneer, Roland Griffiths, shared in an interview: “I do recall one man who had the psilocybin experience. […] He came to believe in the reality of God. And it wasn’t that he was filled with spiritual language – you know, God’s going to save me. No, it was an acceptance for his condition and a reassurance to the people he loved most that everything was as it should be. Everything was OK.”
Psilocybin for Substance Use Disorders
On the addiction front, a 2019 survey22 found that 83% of respondents with a history of alcohol use disorder no longer met the criteria for addiction following a psychedelic experience, with many crediting profound shifts in values and priorities for their reduced drinking. This was followed by a more rigorous 2022 randomized controlled trial23, in which 95 adults with alcohol use disorder received either two sessions of psilocybin-assisted psychotherapy or a placebo. Those in the psilocybin group showed significantly greater reductions in heavy drinking days compared to the placebo group, adding meaningful clinical weight to what the earlier survey data had suggested.
On smoking, a 2014 Johns Hopkins pilot study24 administered psilocybin together with cognitive behavioural therapy to 15 long-term smokers who had averaged six previous failed quit attempts. At six months, 80% were abstinent, a rate far exceeding anything seen with conventional cessation treatments. More recently, a 2026 pilot trial25 found that psilocybin outperformed nicotine patches for smoking cessation, with 40.5% of the psilocybin group having quit at six months compared to just 10% in the patch group.
Across these studies, a recurring theme is that psilocybin’s effect on addiction appears to operate differently from conventional treatments. Rather than simply managing cravings or withdrawal, participants frequently describe a fundamental shift in how they relate to the substance itself, producing shifts in identity, values, and priorities.

Psilocybin for Obsessive Compulsive Disorder
A 2025 study26 from researchers at Imperial College London explored psilocybin as a potential treatment for OCD, a condition that is believed to impact 1 in 40 adults27, with around 30-40% of patients not responding to current lines of treatment28. Nineteen adults with moderate to severe OCD received two doses of psilocybin four weeks apart, receiving an initial very low 1mg control dose followed by a 10mg active dose, accompanied by psychological support before, during, and after each session. Preliminary findings showed that a single 10mg dose produced a rapid-onset, moderately large reduction in OCD symptoms, specifically compulsions, within one week of dosing. Notably, the effect appeared to be independent of any improvement in depression, suggesting psilocybin may act directly on the compulsive mechanisms of OCD rather than simply lifting mood.
The study also found that a lower dose of psilocybin may actually be preferable for OCD patients compared to the higher doses typically used in depression trials. Many people with OCD experience significant anxiety around loss of control, and the 10mg dose produced meaningful symptom relief without the more intense psychedelic effects associated with higher doses. While the effects diminished after the first week with a small sample size, researchers hope to conduct a larger randomized controlled trial, and suggest that combining psilocybin with established OCD therapies such as cognitive behavioural therapy and exposure and response prevention could further enhance outcomes.
Psilocybin for Chronic Pain
Psilocybin for chronic pain is a more novel application of the molecule, with chronic pain affecting millions of people world over. A 2024 review paper29 makes a compelling case for psilocybin as a novel treatment for chronic pain, examining both the emerging clinical evidence and the potential mechanisms by which it might work. The authors propose several overlapping pathways through which psilocybin may reduce pain, suggesting its action on 5-HT2A serotonin receptors in key brain regions involved in both pain and mood regulation may directly modulate how pain signals are processed and perceived. Further, they suggest psilocybin’s neuroplastic effects30 may help reverse the maladaptive brain changes that underlie chronic pain conditions.
Psilocybin also appears to have anti-inflammatory properties31, and by reducing the emotional and psychological burden of pain it may address dimensions of chronic pain that conventional treatments do not. Representing a potential paradigm shift in pain therapy, psilocybin is being explored as a way to help shift a person’s relationship with pain, offering a ‘reset’ in terms of how they conceptualize it.
The early clinical evidence is encouraging, with trials reporting significant reductions in attack frequency and pain severity in people with cluster headaches and migraines13, reductions in pain in post-treatment Lyme disease, and promising case studies in conditions including phantom limb pain32, fibromyalgia33, and long-COVID34.
A pilot feasibility study which has yet to start aims to combine psilocybin with women’s health, specifically exploring whether a single, moderate dose could help women who suffer with chronic pelvic pain, which is thought to affect up to 26% of women globally.
The Psychedelics and Pain Association is an online community and resource base raising awareness for ongoing and past research on the potential of psychedelics to alleviate symptoms in a wide variety of chronic pain conditions.
Psilocybin for Eating Disorders
A 2023 phase 1 feasibility study35 from researchers at UC San Diego was the first clinical trial to investigate psilocybin therapy for anorexia nervosa, administering a single 25mg dose of synthetic psilocybin to ten adult women alongside psychological support. While results were variable across participants, 40% showed clinically significant reductions in eating disorder psychopathology such as fear of weight gain or body image distortion at three-month follow-up, with scores dropping from clinical ranges to within normal values. Participants also reported significant reductions in anxiety, body image distress, and food-related preoccupations. Notably, 90% of participants said one session was not enough, suggesting additional psilocybin experiences may be beneficial.
Another 2023 pilot study36 from Columbia University explored psilocybin for body dysmorphic disorder (BDD), a condition characterized by obsessive preoccupation with perceived flaws in appearance, affecting up to 3% of the general population and has a high rate of suicide attempts37. Twelve adults with moderate to severe BDD who had not responded to treatment with antidepressants received a single high dose of psilocybin with therapeutic support. Their symptoms decreased significantly over a twelve-week period, with improvements also seen in feeling less distressed, less swayed by their negative self-perception, and better able to function day-to-day.
Both conditions are characterized by rigid thinking and a troubled relationship with the body, with psilocybin’s ability to increase cognitive flexibility, loosen fixed beliefs, and occasion profound shifts in self-perception positioning it as a unique line of treatment.


What Psilocybin Therapy Feels Like
Psilocybin-assisted therapy follows three phases: preparation, dosing, and integration, preceded by an initial screening to assess whether someone is a suitable candidate based on their medical and psychiatric history, current medications, and family history.
The preparation phase typically involves one to three sessions with a therapist or facilitator, focused on building rapport, addressing any doubts, and setting intentions. Intention setting serves as a grounding anchor during the session, giving the participant a lens through which to process whatever arises.
Dosing sessions last six to eight hours. The participant is invited to turn inward, usually lying down with eyeshades and carefully curated music, allowing the experience to unfold. Therapists work in a non-directive way, offering minimal interference but remaining present to provide reassurance when needed, whether that is a supportive word or a hand on the shoulder. Protocols typically involve one or two sessions, with two-session models often using an ascending dose structure, starting with a moderate dose before a higher therapeutic dose in the second session.
The most important conversations shaping the future of psychedelics, delivered weekly.
From thought-provoking podcasts and original stories to research breakthroughs and industry news, stay connected to the conversations that matter.
Joined by 12,000+ readers
Integration is the deliberate process of making meaning from the experience, taking insights from the psychedelic state and grounding them in lasting, everyday change. It might involve journaling, mindfulness, movement, or time in nature. Many practitioners argue it is the most important phase of all. As psychedelic researcher Walter Pahnke wrote, “[…] what one does with a psychedelic experience may be more important than merely having it. Without integration […] the experience may be only an irrelevant memory, no matter how beautiful.”
Effects on the Body and Mind
The initial effects come on within 30 minutes to an hour and a half of ingesting it. In this onset period, sensory shifts are common: colors become more vivid, alongside physical sensations such as nausea, tingling, changes in heart rate and body temperature, dizziness, or chills. These tend to be transient and settle as the experience deepens.
The peak, generally between one and a half to four hours in, is where the experience reaches its fullest expression. Perceptual shifts become more pronounced, with significant alterations to the experience of space, time, and self. The peak can also bring profound euphoria, deep introspection, and an expanded sense of empathy and connectedness. If a mystical-type experience occurs, it will typically unfold in this stage, with research suggesting38 it is often here that the most therapeutically significant shifts take place.
It is worth noting that while there are mapped commonalities, every person’s experience is unique. Czech psychiatrist Stanislav Grof described psychedelics as “non-specific amplifiers” of the human psyche, meaning they tend to magnify whatever is already present in a given individual’s conscious and unconscious mind. No amount of preparation can guarantee a particular outcome, which is why cultivating a sense of openness and working with expectations beforehand is paramount.
After the peak, intensity gradually fades, with consciousness slowly reassembling in a new way. In the hours and days that follow, researchers have documented what is often called the “afterglow39”: a state characterized by increased wellbeing, emotional openness, and heightened social connection. Rather than an abrupt return to baseline, it can feel as though the world has been subtly but meaningfully recolored.

Neurologically, the afterglow period is thought to reflect reduced amygdala reactivity and a window of heightened neuroplasticity, in which the brain may be unusually open to change. For this reason, there is growing emphasis in clinical and non-clinical contexts alike on moving slowly in the days following a session, treating this period as a valuable opportunity to intentionally integrate and extend therapeutic benefit.
Even with careful preparation, challenging experiences can still occur. Difficulty or bad trips are characterized by fear, anxiety, paranoia, or feeling trapped in negative thought loops. Ideally, trained facilitators work with their clients beforehand, helping them develop the capacity to sit with uncertainty and emotional intensity.
It is also worth noting that in many Indigenous traditions, difficulty is not considered an unwanted side effect to be minimized, but an integral part of the healing encounter. In traditional Mazatec veladas, for instance, vomiting was considered essential to the ceremony, understood as part of the process of getting well.
Effects on the Mind
- Dissolution of rigid, self-critical thought patterns
- Increased psychological flexibility and openness
- Heightened sense of meaning and purpose
- Heightened sensory perception and visual effects
- Emotional intensity, which can range from profound joy to fear or grief
- Resurfacing of difficult memories or trauma
- Shifts in values and identity
- Improved emotional processing
- Afterglow period of increased wellbeing and social connection
Effects on the Body
- Temporary increases in heart rate and blood pressure during the session
- Nausea during onset, which typically passes
- Fatigue and exhaustion following the session
- Increased neuroplasticity
- Anti-inflammatory effects
Side Effects, Risks, and Contraindications
Psilocybin is considered physiologically safe and non-addictive40. The body builds tolerance quickly, meaning daily use would rapidly diminish its effects, making compulsive use essentially self-defeating.
Even so, it is not without risks. Beyond potential moments of acute discomfort41 during the experience itself, some individuals encounter persisting difficulties afterward, including anxiety42, derealization43, perceptual disturbances44 such as Hallucinogen Persisting Perception Disorder (HPPD), and psychosis-like or manic symptoms. With appropriate support, many of these difficulties resolve over time. The Challenging Psychedelic Experiences Project offers free peer support for persisting difficulties, as does Fireside Project in the US, and ICEERS internationally.
These risks are considerably lower in professionally supported settings, where more care goes into screening, preparation, and integration. Vetting facilitators and therapists thoroughly before working with them is equally important, as inexperience on the part of a guide is itself a meaningful risk factor. It is also worth knowing that psychedelic healing is non-linear, and feeling temporarily worse before noticing improvement is not uncommon.
Contraindications
There are specific circumstances in which psilocybin-assisted therapy is inadvisable, both because research in certain populations is limited and because the field has a responsibility to protect vulnerable groups while the evidence base is still maturing.
Contraindications include:
- Personal or family history of psychosis or schizophrenia
- Bipolar I disorder or significant risk of mania
- Severe cardiovascular disease
- Pregnancy or breastfeeding
- Active suicidal ideation without close medical supervision
- Severe psychiatric instability
- Certain personality vulnerabilities such as dissociative tendencies
Drug Interactions
Medication interactions are also an important consideration. Chronic use of SSRIs or SNRIs downregulates the 5-HT2A receptors45 that psilocybin depends on, significantly blunting the therapeutic experience. This presents a genuine clinical dilemma, as many people seeking psilocybin therapy are currently taking these medications. Tapering off them carries real risks of discontinuation symptoms and mood destabilization, and should never be undertaken without careful medical supervision.
Lithium, the mood-stabilizing prescription medication used primarily to treat and prevent acute manic episodes in bipolar disorder, presents a more serious concern. Combining lithium with psilocybin and other psychedelics has been associated with an increased risk of seizures and cardiac complications46. People taking lithium for bipolar disorder should avoid using psilocybin without explicit medical guidance, and given that bipolar I disorder is itself a contraindication for psilocybin therapy, this combination warrants further caution.
MAOIs (monoamine oxidase inhibitors), an older class of antidepressant, carry a different type of risk. By inhibiting the enzyme that breaks down serotonin, MAOIs can significantly intensify and prolong the effects of psilocybin, and in some cases increase the risk of serotonin syndrome47, a potentially dangerous condition caused by excess serotonin activity, although it is thought that psilocybin carries a lower risk of serotonin toxicity than substances like MDMA. Separately, stimulants such as Adderall and Ritalin may also interact unpredictably with psilocybin, potentially increasing cardiovascular strain or amplifying anxiety during the experience.


Dosage Protocols
Dosing varies significantly depending on context. As previously mentioned, psilocybin is available in several forms, impacting dosing and how the experience unfolds over time. In clinical research settings, pharmaceutical-grade synthetic psilocybin is used. Administered in capsule form, the dose is precisely measured, generally producing more standardized dosing and a predictable onset.
Beyond clinical settings, psilocybin is most commonly consumed as dried mushrooms, either eaten whole, brewed into a tea, or ground into powder in capsules, though the potency of whole mushrooms varies considerably between species, strains, and even individual specimens, making precise dosing more difficult.
Some people also consume fresh mushrooms or truffles (the underground sclerotia48 of the same fungi) particularly in the Netherlands where they are legal, or use mushroom extracts and tinctures. The method of administration also impacts the experience timeline, with synthetic psilocybin in capsule form tending to have a slightly slower and more gradual onset than mushroom tea for example, which is absorbed into the bloodstream more quickly, whilst eating whole dried mushrooms falls somewhere in between.
In clinical settings, synthetic psilocybin is dosed in milligrams, either as a fixed dose or adjusted by body weight. A micro-to-low dose of 1-5mg produces subtle cognitive shifts and mild sensory enhancement without full psychedelic effects. A moderate dose of 10-20mg is likely to produce noticeable visual effects, while 25mg and above is considered a high dose and is the range used in the majority of clinical trials, associated with the strongest therapeutic outcomes and most likely to produce a complete mystical experience.
Outside clinical settings, whole mushrooms are used, which vary considerably in potency. One gram of dried mushrooms is considered a low dose, 1.75-2g moderate, 3g high, and 5g or more a so-called heroic dose.
Additionally, some people choose to microdose, taking a subperceptual amount, typically 0.1 to 0.5 grams of dried mushrooms. Popular protocols include the Fadiman Protocol (one day on, two days off) and the Stamets Stack, which combines psilocybin with Lion’s Mane and Niacin (four days on, three days off). Reported benefits include improvements in mood, creativity, and focus, though the science remains inconclusive49.
Patient Stories
Clinical psychologist Patricia Song, a second-generation Korean immigrant in the US, describes a personal psilocybin experience that helped her connect more deeply with her identity and process intergenerational trauma. During the experience, she found herself feeling profound compassion for her mother, who had lived through the terror and loss of war without ever fully processing her grief.
“I could see all the ways she fought it, and I told her, ‘Yes, you were the best at all these things, you were the most important person in my life,’” Song shared. “I also saw Korea and Koreans as struggling with so much loss. And then everything just vanishes, erodes away, like sand in the wind, by time. It was pretty desolate and dark. But love is the one thing that can endure and love is an act of hope and light.”
“The insights and emotional processing from my journey really helped me continue to work with my grief, to create a companionship with it, although it is a lifelong process. Grief and loss had not been part of my family’s vocabulary and so we all had difficulty with it. These changes, this growth has been permanent and a gift from the medicine work. It has deepened my relationships and experiences of love and loving and of course been a boon to my mental health.”
These experiences point to a recurring theme in psychedelic healing: that transformation rarely happens in isolation. Psychedelic educator and facilitator Mikaela de la Myco speaks from both sides of the healing relationship, describing her experience sitting in a retreat in Jamaica, and advocating for the importance of healing in group contexts.
“I want to speak not only as someone who has provided care to others, but as someone who has also received care from wonderful organizations and communities,” she says. “The work of healing is ongoing and shared by many hands. It takes many of us to create healing spaces, and it takes many to support someone’s journey as those changes take shape over time. I’ve grown a sense of safety in my body, as a participant, by learning how to trust a team of people with my restoration and that sense of safety extends when I work with someone who has a support team in their life — be it therapists and clinicians, family members, a spiritual community or a close group of friends — we do it together. As someone who suffered from crippling social anxiety in the past, learning how to trust people with my care and the care of others has made a huge difference in my life. Healing that wound has come from what I’ve observed, witnessed, and experienced in group healing spaces and ongoing communal care.”
Therapist Stories
Khmer-American trauma therapist, Pai Duch, spoke of the healing benefits of psilocybin that she has encountered first-hand in the communities that she serves. “I have witnessed reductions in suicidal ideation and loneliness, along with increased senses of purpose, belonging, and the capacity for individuals to free themselves from maladaptive coping behaviors,” she said.
Psychedelic facilitator, Gisel Romero, shares:
These medicines are helping us reconnect with the deepest parts of ourselves that modern life has caused us to forget and more importantly, they’re restoring our bond with nature, a disconnection that I believe is one of the most profound dysfunctions of our time.
Psychotherapist and co-founder of Inwardbound psilocybin retreats in the Netherlands, Rob Ó Cobhthaigh, has served over 1,000 people from more than 40 countries in his therapeutic psilocybin retreat process. “I am more convinced than ever of the deep healing potential of this work with psilocybin,” he shares. “I have seen so many lives transformed — some of the darkest traumas and most tragic stories rewritten, processed, and integrated. I believe this work is one of the greatest gifts to humanity.”
Even so, they caution that these experiences are not for everyone. “There are real risks involved, and practitioners and facilitators who hold space have a responsibility to provide informed consent and clearly communicate the potential risks and benefits of these offerings,” says Duch. “My concern is that, in the excitement to push psychedelics forward, we may begin to reduce or overlook important safety protocols, such as comprehensive medical screenings.”
Ó Cobhthaigh also stresses the integrity that facilitators and therapists must have going into this work.
“It requires a willingness on the part of facilitators and therapists to go into the depths with our clients. It requires trust and courage. This work also challenges the therapists and facilitators who hold these spaces in many ways. Everything is amplified in ceremonial spaces, including our own personal shadows, our egos, our power struggles, and our hidden narcissism.”
He also makes a case for the sacredness and mystery of the work. “I always say to our clients that we do not control the outcome. This has been one of the most challenging things for me as a therapist: to surrender control of the outcome.”
Legal Status Worldwide
The legal landscape surrounding psilocybin is one of the most rapidly evolving areas in global drug policy, with growing tension between decades-old prohibitionist frameworks and a body of clinical evidence that regulators are finding increasingly difficult to ignore.
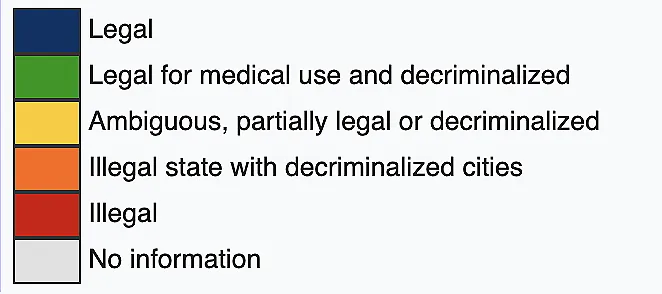
Psilocybin remains Schedule I under the 1971 UN Convention on Psychotropic Substances, though individual countries vary considerably in how they regulate it. In the US, it is still a federal Schedule I substance, though Oregon and Colorado have legalized supervised therapeutic use, and cities including Denver, Seattle, and Washington D.C. have decriminalized personal possession.
Australia became the first country to formally approve psilocybin as a prescription medicine in 2023, for treatment-resistant depression under psychiatric supervision. Canada permits limited access through a Special Access Program50 for serious or life-threatening conditions.
In Europe, the Netherlands has become a hub for psilocybin retreats, even though psilocybin mushrooms are still technically illegal there. Operating through a legal technicality, psilocybin-containing truffles were never explicitly included in the 2008 ban on magic mushrooms, remaining legal to purchase and consume. This legal grey area has allowed a thriving retreat industry to operate openly, with facilitators offering supervised psilocybin experiences to participants from around the globe. While the truffles are legal, they contain the same active compounds as the mushrooms, and the experiences they produce are thought to be functionally identical.
Elsewhere in Europe, Switzerland allows compassionate use under regulatory approval, and Portugal treats personal possession as a public health matter rather than a criminal one. Jamaica is one of the only countries where psilocybin is fully legal, and Mexico permits its use in traditional ceremonial contexts, a provision rooted in the protection of Indigenous biocultural rights.
It is worth distinguishing between decriminalization, which removes criminal penalties for personal possession without legalizing a substance, and legalization, which establishes formal frameworks for supervised use or commercial access.
For those looking to access psilocybin-assisted therapy, options include licensed service centers in Oregon and Colorado, clinical trials such as those run by the Imperial College Centre for Psychedelic Research, compassionate use pathways in Canada and Australia, and retreats in Jamaica, the Netherlands, Mexico, and beyond, though quality and safety vary considerably. Whatever the route, it is important to carefully vet any practitioner51 before proceeding. Many underground practitioners operate with as much care and skill as those in licensed settings, and have long served as a vital form of community care long before legal frameworks existed.

Looking Ahead
Even with all of this positive data about psilocybin and its therapeutic benefits, it is worth pointing out that psilocybin is not legal as an approved treatment. Even so, the clinical landscape continues to unfold. Compass Pathways, a British biotech company, has now successfully met the primary endpoint in both of its Phase 3 trials evaluating COMP360, a synthetic formulation of psilocybin, for treatment-resistant depression, with results across more than 1,000 participants demonstrating consistent, statistically significant outcomes, making COMP360 the first classic psychedelic to consistently achieve this benchmark in Phase 3 trials. As recently as April 2026, the FDA granted Compass a rolling review for its New Drug Application (NDA), reviewing the clinical data as it arrives, rather than waiting for the full application, a process typically reserved for treatments showing strong promise for serious unmet medical needs.
Meanwhile, Usona Institute, a US-based medical research organization, has launched its Phase 3 uAspire trial, a randomized, double-blind, multicenter study evaluating psilocybin in adults with major depressive disorder, enrolling approximately 240 participants across the US. If these trials continue on their current trajectory, FDA approval of psilocybin for depression could be closer than most people realize.
Even with all of these positive therapeutic outcomes and clinical applications, it is worth noting that psilocybin and other psychedelics are not magic bullets or cure-alls. Compared with antidepressants, which are taken daily to manage symptoms, working with psilocybin involves an ongoing commitment to the inner spiritual and psychological work. It is not as simple as passively ingesting a substance and feeling better.
This points to something that sets psychedelics apart from most Western pharmacological approaches: they are considered transdiagnostic, meaning they appear to cut across conditions rather than targeting specific symptoms. Where conventional medicine tends to operate at the level of symptom management, psychedelic healing has long been oriented toward root causes, working on the understanding that mind, body, and spirit are interconnected.