Reading Navigation
Ketamine for Mental Health


Why Ketamine Is Reshaping Mental Health Treatment
Ketamine is not new. It has been in operating rooms and emergency departments for decades. First approved by the U.S. Food and Drug Administration in 1970 as a surgical anesthetic, ketamine became a staple in medicine because of its reliability. It is fast-acting, safe in many contexts, and able to maintain breathing and cardiovascular stability during procedures. For years, its role remained within anesthesia and emergency medicine1.
Then psychiatry paid attention, and over the past two decades, a growing body of research has revealed that ketamine can produce rapid antidepressant effects, particularly in individuals with treatment-resistant depression (TRD) and acute suicidality. Unlike conventional antidepressants ketamine can shift mood and cognitive rigidity2 within hours to days. That temporal difference has motivated clinicians and researchers to reconsider assumptions about how depression can be treated.
This shift is happening in a moment of need. Rates of depression, suicide, and psychological distress have been rising globally, while traditional pharmacological treatments often fall short. Standard antidepressants primarily target monoamine systems3 and tend to work slowly, and often inconsistently or incompletely. Many patients cycle through multiple medications with partial relief.
Ketamine has entered this landscape not as a miracle, but as something psychiatry rarely sees, which is a mechanistically different intervention that might work through alternative neural pathways than traditional antidepressants. Its effects on glutamatergic signaling, synaptic plasticity, and neural network flexibility suggest that the brain may be capable of shifting out of depressive states “more quickly” than previously believed.
The rapid effects of ketamine have generated excitement, yet they demand careful clinical oversight and realistic expectations. Ketamine is not a magic wand that erases suffering, trauma, or the structural conditions that shape mental health. It appears to open a window, one that may temporarily loosen rigid cognitive and emotional patterns, allowing psychotherapy, behavioral change, and relational healing to take deeper root.
What Is Ketamine? Clinical Foundations and Medical Context
Medical History and Classification
Before ketamine became the subject of podcasts, venture capital, and wellness branding, it was (is) a workhorse medication in medicine. Pharmacologically, ketamine is classified as a dissociative anesthetic, meaning it produces a state in which perception, sensation, and awareness become partially uncoupled from one another. Patients remain breathing and physiologically stable while consciousness shifts into a detached or dreamlike state. From a medical standpoint4, this profile is useful as it allows physicians to perform procedures while maintaining cardiovascular stability and protective airway reflexes.
Because of these properties, ketamine became adopted across medical settings after its approval by the U.S. Food and Drug Administration in 1970. It has since been used for decades in surgery, trauma care, battlefield medicine, and pediatric anesthesia, particularly in situations where sedation and safety are essential5. Today, ketamine is included on the World Health Organization List of Essential Medicines, a designation reserved for medications considered fundamental to functioning healthcare systems worldwide.
This historical context matters, because it grounds the current conversation. Ketamine emerged from operating rooms, trauma bays, and emergency departments. The dissociative properties hinted at something more psychologically interesting. By altering perception, interrupting habitual patterns of thought, and temporarily shifting how the brain organizes experience, ketamine creates a state that feels meaningfully different from ordinary consciousness. From a medical perspective, this was pharmacology. From a psychological perspective, it raised a deeper question: what happens when the brain is briefly released from its rigid patterns?
Explore the context
Forms Used in Mental Health
In modern psychiatric care, ketamine is administered through several different routes6, depending on the clinical setting7, regulatory approval status, and treatment protocol.
Common forms used in mental health contexts include:
- IV ketamine (racemic ketamine)
- Intranasal esketamine (an U.S. Food and Drug Administration–approved formulation for treatment-resistant depression) (FDA, 2019)
- Intramuscular (IM) and oral routes used in some off-label clinical settings
These distinctions reflect pharmacological differences and regulatory frameworks that shape how ketamine is used in psychiatric treatment. At the molecular level, traditional ketamine is a racemic mixture, meaning it contains two mirror-image molecules: R-ketamine and S-ketamine. Standard IV ketamine used in most clinical protocols contains both of these forms together. In contrast, esketamine refers specifically to the S-enantiomer of the molecule8, which was isolated and developed as a proprietary intranasal medication. This formulation was approved by the U.S. Food and Drug Administration in 2019 for treatment-resistant depression and must be administered within a structured clinical program with monitoring requirements.
The distinction also highlights an important regulatory concept in medicine: on-label versus off-label prescribing.
- On-label use refers to medications prescribed exactly as approved by regulatory agencies such as the FDA (meaning the drug, dose, route of administration, and clinical indication match the original approval).
- Off-label use refers to prescribing an approved medication in a way that differs from its official indication or formulation but is supported by emerging evidence or clinical practice.
In the case of ketamine, intranasal esketamine represents the primary FDA-approved psychiatric formulation, while many IV, IM, and oral ketamine protocols used in depression treatment operate under off-label prescribing. This regulatory landscape can sometimes create confusion in public discussions about ketamine.
The Mental Health Treatment Gap: Why Innovation Is Needed
Most antidepressant medications prescribed today operate on a similar biological premise: they modulate monoamine neurotransmitters such as serotonin, norepinephrine, or dopamine. These medications can be effective for many individuals, and for some they are life-changing. But a substantial proportion of patients do not experience full relief.
Research suggests that approximately one-third of individuals10 with major depressive disorder (MDD) meet criteria3 for treatment-resistant depression (typically defined as failing to respond adequately to two or more antidepressant trials). Even among patients who do experience improvement, complete remission is far from guaranteed, and many individuals continue to struggle with residual symptoms.
Traditional antidepressants typically require four to eight weeks before a meaningful therapeutic response can be evaluated. For clinicians and patients alike, this delay creates a difficult dynamic11: treatment decisions must be made while symptoms remain active, often severe, and sometimes life-threatening. Medication trials become slow-moving experiments conducted in real time while a person is still suffering. This delay introduces what some researchers describe as treatment latency or the period between initiating a treatment and experiencing relief. From a public health perspective, treatment latency is not just an inconvenience, but it can be a period of heightened vulnerability12.
During medication transitions (when individuals are starting a new antidepressant, tapering another, or waiting to see whether a drug will work) patients may remain in states of severe depression. Clinicians know this tension well: we are often asking people to endure weeks of uncertainty while hoping the brain will eventually respond. At the same time, the broader landscape of antidepressant development13has changed little over the past several decades. This context helps explain why ketamine has attracted such scientific interest, because it appears to operate through different neurobiological pathways.
How Ketamine Works in the Brain: Beyond the Monoamine Model
For decades, the dominant biological explanation for depression centered on monoamines14 (serotonin, norepinephrine, and dopamine). The theory was pharmacologically opportune: if depression reflected a deficit in these neurotransmitters, then medications that increased their availability should improve mood.
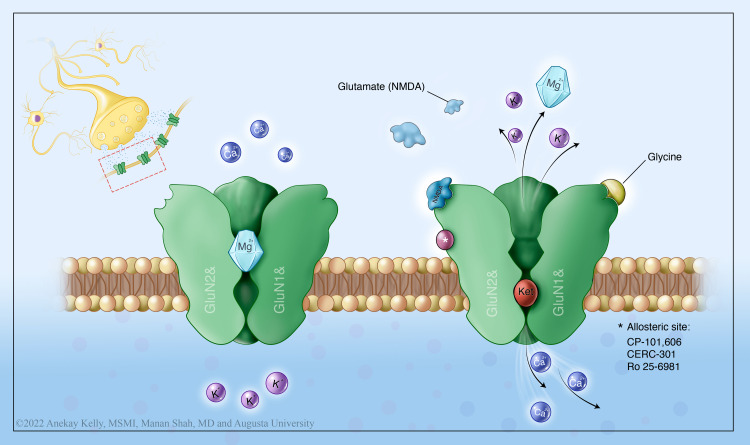
Emerging research suggests15 that the disorder may also involve disruptions in glutamate signaling, neural plasticity, and the brain’s ability to adapt to stress and experience. Rather than targeting serotonin reuptake or dopamine metabolism, ketamine acts primarily as an NMDA receptor antagonist16, altering the activity of glutamate (the brain’s abundant excitatory neurotransmitter). In simple terms, ketamine temporarily interferes with a specific receptor that normally regulates excitatory signaling within neural networks.
Chemical messengers (neurotransmitters) in the brain including serotonin, norepinephrine, and dopamine. They regulate mood, sleep, appetite, focus, motivation, and emotional responses. The brain produces and releases monoamines to communicate between neurons.
NMDA Receptor Antagonism
Ketamine blocks NMDA receptors, triggering a cascade that increases glutamate release and enhances signaling through AMPA receptors17 (mechanisms thought to underlie its rapid antidepressant effects).
A protein channel on the surface of brain cells that receives chemical signals. When activated by the neurotransmitter glutamate, it allows ions (particularly calcium) to enter the neuron, triggering electrical activity and cellular responses. NMDA receptors are especially important for learning and memory formation.
This creates a brief but meaningful shift in brain activity, especially in regions involved in mood, cognition, and emotional processing like the prefrontal cortex. At a systems level, this disruption can loosen rigid neural patterns seen in chronic depression. Brain networks stuck in loops of rumination or emotional shutdown may become temporarily more flexible (what neuroscientists call increased plasticity, or the brain’s capacity to update its internal models). Depression often feels like psychological gravity18, pulling the mind toward the same thoughts and emotional conclusions.
Ketamine appears to interrupt that pull, creating a window where entrenched patterns can shift more quickly. In doing so, it temporarily destabilizes the neural architecture of depression, making meaningful change (biological, psychological, and behavioral) more possible.
Synaptogenesis and Neural Plasticity
One of the more widely studied downstream effects of ketamine involves brain-derived neurotrophic factor (BDNF). BDNF is a protein that helps brain cells grow, connect, and communicate. In depression and trauma, BDNF levels are often lower.
A protein in the brain that supports the survival of existing neurons and encourages growth of new neurons and synapses. Acts as a growth factor, promoting the development of new nerve cells and strengthening connections between them. Essential for learning, memory, and neural adaptation.
Chronic stress can lead to reduced connectivity, especially in areas like the prefrontal cortex and hippocampus, which are important for emotion regulation, memory, and flexible thinking. This is part of why people can feel stuck in the same patterns of thought and emotion. Ketamine appears to increase BDNF by boosting glutamate activity in the brain. This activates cellular pathways (including the mTOR pathway) that tell neurons to start building new connections.
The key idea is that BDNF supports neuroplasticity, or the brain’s ability to adapt, update, and form new pathways. When BDNF increases, the brain may become less rigid and more flexible, creating a window where new patterns (emotional, cognitive, behavioral) are easier to form. For a full review of signaling pathways, see Duman et al., 201120.
Default Mode Network and Rumination
Another emerging area of ketamine research focuses less on individual neurotransmitters and more on large-scale brain networks (particularly the Default Mode Network (DMN)). The DMN is a group of brain regions active when we’re turned inward, thinking about ourselves, reflecting on the past, or imagining the future. It plays a key role21 in self-awareness and meaning-making. In depression and trauma, the DMN often becomes overactive and overly connected.
This can show up as rumination22, self-criticism, and repetitive negative thinking, like the brain is stuck replaying the same painful story on a loop. Ketamine appears to temporarily disrupt this pattern. Research suggests it reduces rigid connectivity23 within the DMN while increasing communication with other brain networks involved in flexibility and emotional regulation. The brain may loosen its grip on the same narrative, creating space for new perspectives and experiences to emerge.
A set of interconnected brain regions that become active when the mind is at rest or turned inward — during self-reflection, recalling memories, imagining the future, or thinking about oneself. Includes areas like the medial prefrontal cortex and posterior cingulate cortex. Active during introspection and autobiographical thinking.

Effects on the Mind (Psychological / Experiential)
Rapid reduction in suicidal thinking
- One of the most robust findings: suicidal ideation can decrease within hours
- Effects may persist days to weeks in some patients
Reduced depression intensity / “mental heaviness”
- Rapid antidepressant effects compared to traditional medications
Decreased rumination and cognitive rigidity
- Patients often report less looping, self-critical thinking
- Linked to changes in large-scale brain networks (e.g., DMN)
Increased cognitive flexibility / perspective shifting
- Greater ability to consider new interpretations or possibilities
- Often described as “mental space” or “less stuckness”
Enhanced emotional access or processing
- Especially in ketamine-assisted psychotherapy (KAP) settings
- Can allow engagement with trauma or avoided material in a new way
Effects on the Body (Neurobiological / Physiological)
Increased neuroplasticity
- Boosts glutamate signaling → increases BDNF → promotes new neural connections
- Supports the brain’s ability to adapt and change
Rapid changes in brain connectivity
- Disrupts rigid network patterns (e.g., overactive self-referential circuits)
- Increases cross-talk between cognitive and emotional regulation systems
Stress-system modulation
- May reduce the intensity of stress-response signaling over time
- Potential downstream effects on how the nervous system responds to threat
Short-term physiological effects during treatment
- Mild increases in heart rate and blood pressure
- Altered sensory perception (dissociation, time distortion)


Duration of Effect
One of the most clinically interesting and sometimes misunderstood features of ketamine treatment is how quickly its effects can appear24. In many patients, improvements in mood, cognitive flexibility, or suicidal ideation may emerge within hours to days25 following administration. For individuals who have spent years waiting weeks for each medication trial to show results, that shift in timeline can feel surreal. But rapid onset does not mean permanent resolution.
In clinical settings, ketamine for depression is often delivered as a series of treatments rather than a single intervention. A typical course may involve multiple infusions26 or administrations over several weeks, allowing cliniciansto build and stabilize the therapeutic response27. The goal is not simply a brief lift in mood, but the gradual consolidation of improvement28 over repeated sessions. Even with an initial response, the duration of benefit can vary considerably between individuals. Some patients experience symptom relief that persists for weeks or months, while others notice that improvements begin to fade more quickly.
Because of this variability, many treatment protocols incorporate maintenance strategies, often referred to as booster sessions. These sessions are administered periodically after the initial series to help sustain symptom relief and prevent relapse. The timing of boosters is typically individualized29, based on the patient’s response pattern and clinical needs rather than a rigid schedule.
Depression is rarely the result of a single biological mechanism, and meaningful recovery often requires multiple layers of support. Psychotherapy, behavioral changes, social connection, and sometimes additional medical care. Ketamine may open a window in which these processes become easier to engage, but the window itself does not stay open indefinitely. For some patients, ketamine may become an intermittent medical support within a broader treatment plan. For others, it may provide a temporary shift that helps catalyze longer-term psychological change.

Realistic Expectations
It is important to remember that ketamine is not universally effective. While many individuals experience meaningful improvement, others show only partial benefit, and some do not respond at all. The variability is not surprising, as depression itself is not a single disorder with a single biological cause. It is a constellation of biological vulnerability, developmental history, relational experience, and environmental stressors. No medication, however novel, is likely to resolve all those layers at once.
This is why ketamine tends to work better within structured treatment plans rather than as a standalone intervention. One of the most important elements of these plans is psychotherapy integration30. When neural plasticity increases, patients may temporarily experience31 greater emotional openness, cognitive flexibility, or capacity to reflect on previously avoided material. Psychotherapy can help translate32 that window of flexibility into meaningful psychological change (examining long-standing beliefs, relational patterns, trauma histories, and behavioral habits that contribute to depressive cycles).
Without that integration, the experience risks remaining primarily pharmacological rather than transformative.
Clinical response can also be influenced by comorbid conditions and individual patient factors. Co-occurring disorders such as PTSD, anxiety disorders, substance use concerns, or personality-related patterns may shape both the experience of treatment and the durability of outcomes. Some individuals respond rapidly, while others require a more gradual and carefully structured approach. Researchers are still working to identify predictors of response33 (the biological, psychological, and environmental variables that help determine who benefits most from ketamine-based treatments).


Safety, Risks, and Clinical Considerations
Clinical Safety Profile
Like any medication that alters brain function, it carries both therapeutic potential and physiological risk34. Ketamine can temporarily increase blood pressure and heart rate, which means patients receiving treatment are routinely monitored during and after administration. Standard protocols typically include measuring vital signs such as blood pressure, heart rate, and oxygen saturation, as well as observing a patient’s psychological response during the experience. In responsible clinical settings, patients are monitored35 throughout the session and remain under supervision until the acute effects of the medication have subsided.
Ketamine is also classified as a Schedule III controlled substance under the U.S. Drug Enforcement Administration. This designation reflects two realities that can coexist: the drug has legitimate medical uses, and it also carries the potential for misuse when taken outside appropriate medical contexts. The classification means the drug requires responsible prescribing and regulated handling. Responsible ketamine treatment occurs within licensed clinics, hospitals, or medical practices where clinicians can monitor safety, screen patients appropriately, and integrate the experience into broader therapeutic care.
Short-Term Side Effects
During the acute phase of treatment, patients may experience several temporary side effects. These effects typically emerge36 during the medication session and resolve as the drug metabolizes.
Common short-term effects include:
- Dissociation, often described as feeling detached from the body, thoughts, or surrounding environment
- Nausea or mild gastrointestinal discomfort
- Elevated blood pressure and heart rate during the active medication period
- Transient perceptual changes, such as altered sensory perception, visual distortions, or dreamlike experiences
For many patients, these experiences are brief and manageable within a clinical environment. However, because ketamine can alter consciousness and perception, sessions are conducted with medical monitoring and supervision to ensure safety throughout the experience. Importantly, dissociation is not inherently harmful, but it can feel unfamiliar or unsettling for some individuals. Preparation, clinical support, and a calm treatment environment are therefore components of responsible care.
Long-Term Risks
While ketamine has been used safely in medicine for decades, long-term data on repeated psychiatric dosing protocols are still evolving37. Most clinical research has focused on short-term treatment courses or follow-up periods of several months. Concerns about long-term risk largely stem from observations in chronic high-dose recreational use, where repeated exposure has been associated with potential complications such as bladder irritation, cognitive changes, and tolerance. These patterns appear primarily in contexts involving frequent, unsupervised, and high-dose use. Nevertheless, the psychiatric field remains appropriately cautious. Questions about long-term durability, optimal dosing schedules, and cumulative exposure are still being actively studied.

Contraindications
Because ketamine affects cardiovascular and perceptual systems, certain medical and psychiatric conditions may make treatment inappropriate38 or require heightened caution.
Common contraindications or areas requiring careful evaluation include:
- Uncontrolled hypertension or significant cardiovascular instability, due to ketamine’s temporary effects on blood pressure
- Active psychotic disorders, where dissociative effects could potentially exacerbate symptoms
- Substance misuse concerns, particularly when patterns of compulsive use or addiction vulnerability are present
For these reasons, most clinics conduct comprehensive medical and psychiatric screening before initiating treatment. As with many psychiatric interventions, safety is not only about the drug alone but about how, where, and for whom it is used.
Importance of Structured Care
One of the important determinants of ketamine’s safety and effectiveness is the context in which it is delivered. The medication itself is only one part of the treatment. Responsible ketamine treatment typically begins with comprehensive medical and psychiatric screening. Clinicians assess cardiovascular health, psychiatric history, medication interactions, substance use patterns, and overall treatment goals. The purpose of screening is not simply to decide whether someone qualifies for ketamine, but to determine whether the treatment can be delivered safely and meaningfully for that patient.
During treatment, structured monitoring protocols are standard. Because ketamine can temporarily elevate blood pressure and alter perception, vital signs are typically observed throughout the session. Patients remain under supervision until the acute effects of the medication have subsided and they are physiologically stable.
Read more about safety protocols
Equally important is integration support. Ketamine may increase emotional openness or cognitive flexibility for a period following treatment. Psychotherapy or structured integration sessions can help patients process insights, shifts in perspective, or emerging emotions so that the experience contributes to longer-term change rather than remaining an isolated altered state.
This structured model of care becomes important in a landscape where ketamine services have expanded rapidly. The medication can be powerful, but the therapeutic value of ketamine often depends on the clinical structure surrounding its use (careful screening, medical monitoring, and thoughtful psychological integration).
Integration and Adjunct Therapies
As we have established, the pharmacology of ketamine may act quickly, but the psychological changes that sustain recovery tend to unfold gradually (and often require intentional therapeutic support). This is where ketamine-assisted psychotherapy (KAP) and structured integration work enter the picture.
In ketamine-assisted psychotherapy models, the medication is administered within a broader therapeutic framework. The ketamine session is not treated as a standalone event but as one component of a larger process that includes preparation, guided experience, and post-session integration. Therapists help patients explore emotional material that may arise, translate insights into daily life, and examine the relational and cognitive patterns41 that contribute to ongoing distress.
Ketamine may temporarily loosen rigid patterns of thinking or emotional avoidance, but those shifts are often fragile unless they are anchored within conscious reflection and behavioral change. Integration sessions provide space to process the experience and ask practical questions: What felt different? What became more visible? What might change now that the system is slightly less stuck?

In many cases, clinicians also encourage behavioral activation following treatment. When depressive symptoms begin to lift, patients may find it easier to engage in activities that support long-term recovery: movement, social connection, creative expression, or re-engagement with meaningful goals. These actions can reinforce the neural changes initiated during treatment.
Some researchers refer to this period following ketamine administration as a “neuroplasticity window.” During this window, the brain may be more capable of forming new connections and updating entrenched cognitive patterns. While the exact duration and mechanisms are still being studied42, the idea is straightforward: when the brain becomes temporarily more flexible, psychological learning may occur more readily.
Which brings us to a point that is sometimes lost in public discussions of ketamine:
The medication may increase receptivity to therapy, but it does not replace therapy.
Ketamine may open the door. The therapeutic work still happens inside the room.
The Future of Ketamine in Mental Health
Ketamine’s rapid antidepressant effects have sparked a wave of scientific interest that extends far beyond the drug itself. Researchers are now asking broader questions about how depression works in the brain, why certain treatments fail, and how neuroplasticity might be harnessed more effectively in psychiatric care. While the field is still evolving, several key areas of research are beginning to shape the future of ketamine-based treatments.
Other Mental Health Conditions Where Ketamine Is Being Studied
- Post-Traumatic Stress Disorder43 (PTSD)
- Anxiety Disorders: Generalized Anxiety Disorder44 (GAD) & Social Anxiety Disorder45
- Obsessive-Compulsive Disorder46 (OCD)
- Substance Use47 & Addictive Disorders48
- Bipolar Spectrum49
- Chronic Pain Disorders50 (Niesters et al., 201450)
- Eating Disorders51
- Borderline Personality Disorder52
Areas Needing More Research
Despite the excitement surrounding ketamine’s clinical potential, significant gaps in knowledge remain. Important areas requiring further research include:
- long-term safety data for repeated psychiatric dosing
- larger and more rigorous clinical trials
Biomarkers and Predictors of Response
Current studies are exploring potential biomarkers and predictors53 of treatment response, including genetic variations that influence glutamate signaling and synaptic plasticity. Some researchers are also examining patterns in electroencephalography (EEG) and functional neuroimaging that may predict how an individual’s brain networks respond to ketamine. The goal is to move toward a more precision-based model of psychiatry, where clinicians can identify patients who are biologically most likely to respond before treatment even begins.
Optimization of Dosing Protocols
Another major area of investigation involves determining how ketamine should be administered36 over time. Clinicians are still working to refine optimal treatment schedules54, including:
- whether personalized scheduling based on symptom return may be more effective than standardized protocols
- the ideal number of sessions during an initial treatment course
- maintenance frequency needed to sustain symptom improvement

Psychedelic Research Crossover
Ketamine research55 has also contributed to a broader resurgence of interest56 in rapid-acting neuroplastic agents57 within psychiatry. This broader research landscape includes renewed scientific attention to compounds such as Psilocybin and MDMA, both of which are being studied for treatment-resistant psychiatric conditions. While these substances differ pharmacologically from ketamine, they share a common scientific question: can certain interventions temporarily increase the brain’s capacity for psychological change?
Therapist perspective
As a Ketamine clinician, I didn’t come into this work because I believed in a miracle solution.
I kept hearing the same pattern: people doing everything they were “supposed” to do (e.g., showing up, doing the work, gaining insight) and still feeling stuck. There was a mind-body disconnect. They had the language, the awareness, the effort, the insights. But something wasn’t shifting. In the right context, certain interventions can open a door. But what I’ve come to believe is what happens after that door opens can be the difference between insight and real-life change. Change is difficult, uncomfortable, and requires real behavioral shifts.
This work often exists in complex settings, with individuals navigating layered and longstanding challenges. It’s rarely simple, and it’s never just one thing. The intervention itself is only one part of a much larger process. I tend to frame these approaches not as fixes, but as catalysts (something that can disrupt patterns, loosen rigidity, and create space for something different to emerge), but this requires desire to change or intrinsic motivation. In fact, one of the biggest “yellow flags” is overestimating the intervention and underestimating one’s unique part in the process – ownership and willingness to look inward. Active, as compared to passive, participation in healing is crucial.
A core part of the process is preparation, or shifting from a passive mindset (“this will fix me”) to a more active one (“how do I want to meet my life differently?”). This often involves exploring many topics, including values, expectations, and the reality that change is rarely linear. During the experience itself, people may encounter a wide range of internal material (emotional, disorienting, meaningful, or difficult to articulate). I believe the role of the clinician isn’t to define that experience, but to help create a space where it can be held and eventually understood as a mechanism to move forward in one’s life in a different direction. Because without a therapeutic container, powerful insight can possibly feel disorienting or fade quickly. Which brings us to an important part of the work: integration.
Integration is the process of asking: What did this reveal? What does it mean? What needs to shift? And what am I actually willing to do differently? It’s not abstract: it’s about translating insight into real life. This is where deeper emotional and relational patterns meet behavior. Change shows up in actions, relationships, boundaries, and habits. Because insight without action often becomes another form of staying stuck (just a more sophisticated kind of intellectualization). I’ve found this work to be more effective when it’s grounded in approaches that support meaningful, sustained change: evidence-based models that help people build psychological flexibility, regulate emotions, and stay connected to themselves and their lives (such as mindfulness-based approaches, cognitive behavioral therapy, acceptance and commitment therapy, and dialectical behavior therapy).
Over time, I’ve shifted away from a purely symptom-focused lens toward something broader. Not just “feeling better,” but living more fully, more connected, more intentional, more aligned. That doesn’t happen in a straight line. There are setbacks, returns to old patterns, moments of clarity followed by confusion. Sometimes even improvement can feel destabilizing (especially when long-held identities or ways of coping begin to shift).
It can be a bit like learning to drive a high-performance car. You suddenly have access to more speed, more responsiveness, more range. But without practice, that power can feel overwhelming or hard to control. With time, though, it becomes something you can navigate with increasing confidence and intention.
That’s why the ongoing work matters. Certain experiences can create insight. But it’s what people do with that insight that creates change. With the right support (through connection, co-regulation, and the experience of being seen and held in a therapeutic relationship) these moments don’t just stay as insight, they begin to reorganize something deeper. Patterns shaped in earlier relationships can start to shift as new experiences are felt, not just understood. In that way, they can become something more enduring. A turning point.
Patient perspective